Now Reading: eHealth: Are you ready to go digital?
-
01
eHealth: Are you ready to go digital?
Naturally, concern for human health is not the only reason for such global changes. The fact is that global healthcare has faced several serious and increasingly aggravating problems in recent years. The world’s population keeps growing, and so does the percentage of the elderly. By 2030, there will be 656 million people over 65 (11.5% of the total population) on the planet, which logically means a spike in healthcare costs. 7.83 trillion dollars was spent on healthcare and medicine around the world in 2013, but the projected amount for 2040 is 18.28 trillion dollars.
In contrast to this increase, the number of medical professionals in all specialties and of all levels is declining evert year. According to the information disseminated by PricewaterhouseCoopers in 2019, about 40% of the world’s positions in healthcare would be vacant in the next 10 years.
To cope with all these problems, healthcare has no choice but to resort to digital technology innovation. Only analysis and synthesis at the speed of light can help us overcome the difficulties ahead.

Robot and human hands almost touching – 3D render. A modern take on the famous Michelangelo painting in the Sistine Chapel; titled, “The Creation of Adam”.
Healthcare 2030: Trends
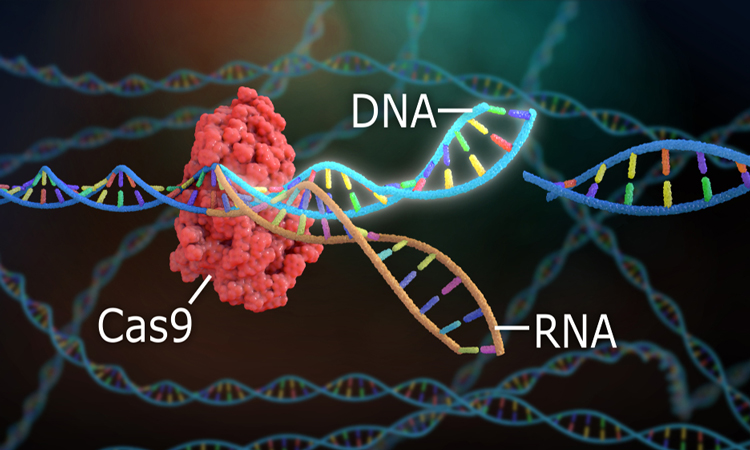
Gene scissors (CRISPR-Cas9): We already can optimize the genetic code of almost all living cells and organisms, and the entire world medicine is waiting for this technology to revolutionize the treatment of cancer and many hereditary diseases.
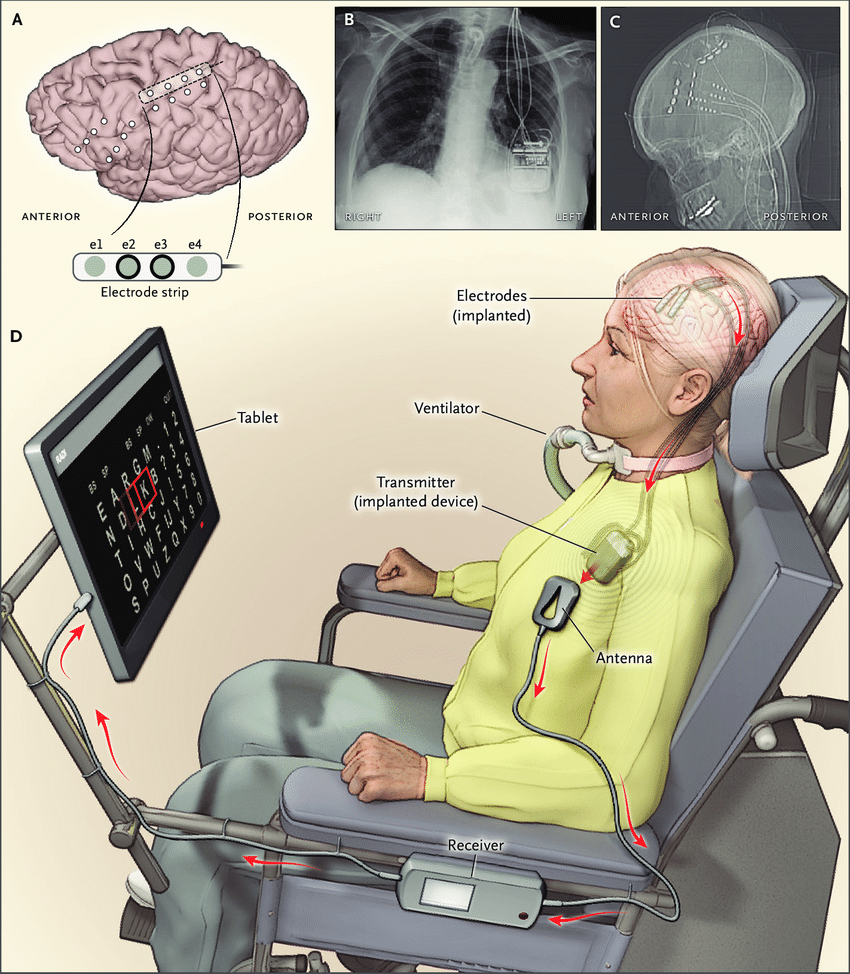
Brain-Computer Interface: These systems are normally implanted neurosurgically in specific centers of the brain, read brain signals and transmit them to a separate device or exoskeleton (for example, a robotic arm, individually designed for a person who has lost an arm in an accident). Similarly, people with speech, hearing or vision problems will also be able to communicate, hear and see with the help of these systems.
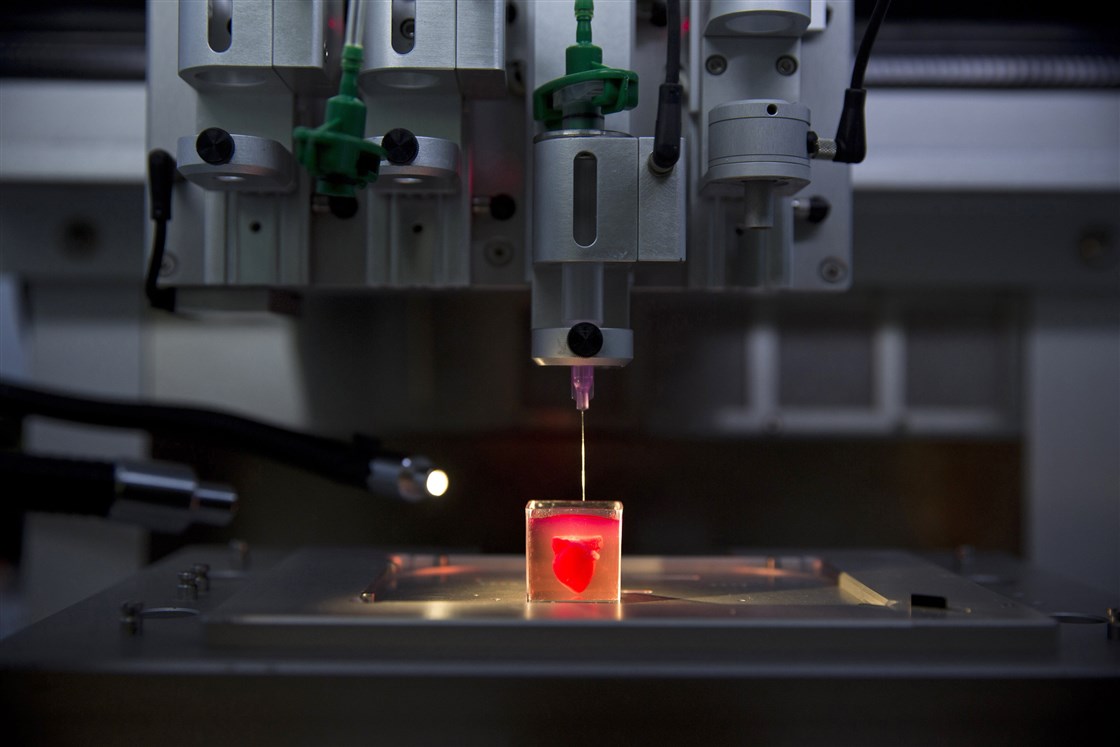
3D cell printing or bioprinting: In the future, this technology will make it possible to synthesize human organs by creating them from living cells using 3D printing. Last year, scientists at Tel Aviv University presented to the public the world’s first small heart “printed” in this way—with all the veins, chambers and nerve fibers. To do this, they first took human fatty tissue cells and reprogrammed them to become stem cells, which they mixed with a special hydrogel and developed the mixture to get heart cells. Then a special 3D printer printed a heart from this “bioink”.

Robotics: The use of robots for various purposes in the treatment and care of patients in nursing homes and rehabilitation clinics is gradually becoming common in many countries. In countries where the elderly population is growing and there is a shortage of staff (for example, in Germany), there is an urgent need for support systems that could replace medical professionals or make their work much easier.
On the one hand, the Japanese have long been using humanoid robots as medical or everyday assistants. On the other hand, Western European society is very skeptical about them: in particular, the application of robotics in social and emotional spheres causes heated ethical discussions. So far, the compromise agreement is that in medicine, the application of robotics should be resource-based rather than deficiency-based. Simply put, robots should not directly replace human interaction, but act as additional intermediaries in it.
Various ethics commissions still believe that it is wrong to use robots to meet the social and emotional needs of people in need of medical care. Their main reasoning is that plastic cannot replace human communication and care.
Robotics used in healthcare can be divided into three groups:
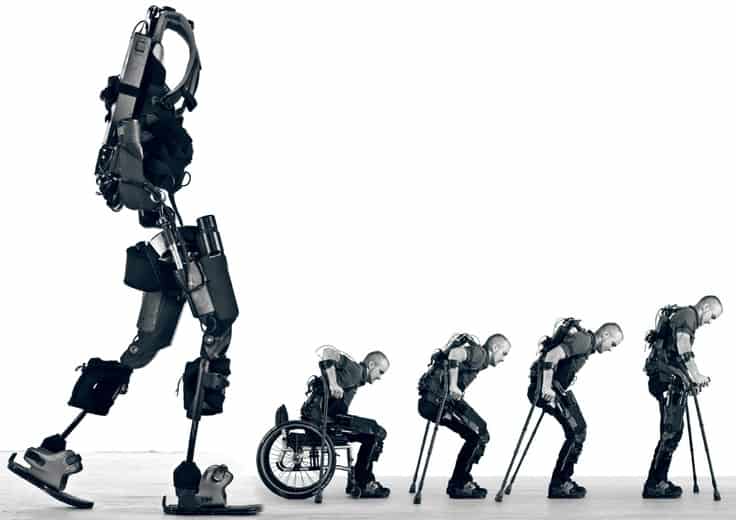
– Assistant robots: devices designed to support the everyday activities of nursing staff and patients. Such devices include, for example, smart beds that help staff lift heavy patients, or exoskeletons that allow patients with limited mobility to move around.


– Monitoring devices: they constantly monitor patients’ vital signs (pulse, respiratory rate, heart rate, blood pressure and blood sugar) remotely and if the indicators go beyond the normal range, they call an ambulance and provide first aid recommendations.
– Social assistance robots: these robots come in a variety of forms, from small toys to medium-sized home assistants. Their main function is to meet the emotional needs of lonely people. One of these robots is the very popular plush baby seal Paro. Contrary to expectations, Paro already works very effectively in nursing homes. Everyone—both medical staff and patients—is happy with the results. According to preliminary observations, Paro has a positive effect on stress, anxiety, depression and sleep disorders in 70-80% of patients, which in most cases leads to reduced prescription of sedatives and sleeping pills.
Research and observations on this topic show that social robots have a calming and stress-reducing effect on patients suffering from dementia.
Artificial Intelligence, Telehealth, Wearables, Augmented Reality, Virtual Reality…
Contrary to initial doubts, telehealth, or telemedicine, which needs no introduction, is becoming increasingly popular with doctors. SARS-CoV-2 gave a great impetus to this process. Patients who cannot physically come to doctors’ offices or clinics due to the risk of infection have to contact them through video calls, and even the most skeptical doctors have to resort to this method.
Today, patients, in particular, the elderly or physically challenged, in many Western European countries regularly contact their family doctors via video calls to address their complaints and questions directly to the attending physician. In the not-too-distant future, “smart watches” on patients’ wrists and other wearable devices will inform doctors in advance about the vital signs of patients, and thus control over treatment will shift even more to another plane.
The introduction of electronic health records will free healthcare professionals from the burden of duplicate documentation and patients from the need to undergo unnecessary repeated examination. Each patient will be able to carry their health records in their pocket—in their smartphone. No more turning the whole apartment upside down in search of the ECG or tomography results from years ago.


Before the World Health Organization, the threat of the SARS-CoV-2 pandemic was announced by the Canadian start-up BlueDot using artificial intelligence.
Artificial intelligence is also able to identify many cause-and-effect relationships previously unknown to medicine. For example, one of the problems in the treatment of depression is the choice of antidepressants. Psychiatrists have long known that the same antidepressant prescribed for the same depressive syndrome does not have the same therapeutic effect on different patients. The choice of an antidepressant is still most often based on the side effects of the drug, or even made by a very simple “trial and error” method. In an interesting study at the University of Southwestern Texas, patients with depression were divided into two groups and given either sertraline (an antidepressant) or a placebo. The researchers monitored changes in the symptoms in both groups for eight weeks, entering all patients’ medical records, especially electroencephalograms (EEGs), in an artificial intelligence program. As a result, the software found a link between a positive response to the antidepressant and patient’s EEG, and was able to determine with 65% accuracy on which patients the drug would have a positive effect, and on which a negative one.
In a similar study at the University of California, machine learning algorithms were used to diagnose Alzheimer’s disease using FDG-PET (FluoroDeoxyGlucose Positron Emission Tomography) images 6 years before its onset.
And this is just the beginning of the journey. In the next decade, artificial intelligence will be able to identify even the rarest genetic disorders by their characteristic appearance. It is the rarity of such disorders (Mabry syndrome, Kabuki syndrome) that makes them difficult to diagnose for many doctors.
Augmented Reality (AR) and Virtual Reality (VR) devices are familiar to all of us thanks to gaming and entertainment, and we can easily imagine the role of these technologies in education. When we were medical students, we would be taken to the surgery department to watch a surgery and seated on special chairs so that we could observe the surgeon’s work from above. Even so, more often than not, we could not see what the surgeon was doing. Now, with VR glasses, medical students in the West can have a first-person view of a surgery—looking through the surgeon’s eyes.
According to a study by the Harvard Business Review magazine, the performance of surgeons trained with VR technology is 230% higher than that of surgeons who received a traditional education.


Wearables are “wearable” devices equipped with various sensors: it can be a smartwatch that measures pulse, blood pressure, body temperature, oxygen saturation in the blood, and even take an ECG and other medical parameters (e.g., Fitbit Ionic, KardiaMobile6L), or a headband that enhances the quality of meditation and sleep (e.g., Muse headband).
We hear so much about nanotechnology that sometimes it seems like an already irrelevant subject, although the main benefits of nanotechnology are only starting to appear on the medical horizon. In 2014, the Max Planck Institute for Intelligent Systems developed remote-controlled microrobots that can move in the blood and other body environments. And Pillcam is a non-invasive examination method currently used in gastroenterological practice. In late 2018, MIT (Massachusetts Institute of Technology) created an electronic remote-controlled diagnostic “pill” that also delivers drugs into a specific part of the body.
https://www.youtube.com/watch?v=VohGE85BlyY
What competencies should the doctor of the future have?
For the new technologies to make an impact on the world of medicine, doctors themselves have to master these technologies first. This is why university clinics, which conduct more studies than research organizations, more and more often expect their potential employees to know statistical software such as Matlab, SPSS, R or other programs and programming languages. A residency in clinical informatics has been offered in the United States since 2013. Its goal is to train doctors specializing in this field, because only healthcare workers themselves can determine what is the most important to them in their daily activities, and thus create the most efficient digital infrastructure for healthcare.

Conclusions
Healthcare in general and the doctor-patient relationship in particular are on the verge of a major paradigm shift. The centuries-old opinion that “the patient does not and cannot know anything important about their illness” has long been a thing of the past. With the help of Dr. Google, patients today can learn about any pathology as much as medical professionals. And this makes a patient’s rightful participation in decision-making regarding the diagnosis and the treatment process inevitable. This is not only a technological, but also a cultural transformation. A doctor should think twice before telling a patient to stay away from the Internet and not to believe the things they find there. This may only cause the patient to stay away not from the Internet, but from that doctor. We must once and for all accept that patients still get information about their health and illness on the Internet, and this trend is on the rise. It would be more appropriate to guide them—for example, by telling them which source is more reliable.
Very soon, many areas of healthcare, especially disease prevention and treatment monitoring, will gradually move from clinics to patients’ homes or offices.
Investors seeking to introduce new technologies in medicine are faced with a challenge they do not encounter in industry, transport or energy: for some reason, healthcare is unable to adapt to technological innovation quite as quickly as expected. Oddly enough, the main obstacle here is medical professionals themselves. Medicine is a system with an extremely rigid hierarchical structure. In other words, those with the status and the position to propose and apply innovations are people who have devoted years of their lives to medicine, recognized veteran specialists in their field over the age of 55-60. When they were studying and gaining experience, there was not even a sign of the technical achievements of recent years, and most older doctors consider these innovations “toys”, refusing to take them seriously.
In his autobiography (Scientific Autobiography and Other Papers), Max Planck, the Nobel laureate in physics, writes how entrenched systems resist change: “A new scientific truth does not triumph by convincing its opponents and making them see the light, but rather because its opponents eventually die, and a new generation grows up that is familiar with it.”
Another problem is that doctors lack business, management and administration skills. It is easy to see where this trend will lead: already increasingly commercialized, losing its humanistic origins, medicine will fall into the hands of “tech monsters”. It is no coincidence that Google spends more and more millions each year on the health and healthcare sector.
Jack Welch, the former chairman and CEO of General Electric, said, “When the rate of change on the outside exceeds the rate of change on the inside, the end is near.” Digitization-wise, today’s healthcare is lagging far behind all other areas. Let us hope that Welch meant large business corporations and his saying does not apply to healthcare.
Aze.Media
Sources:
https://www.wired.com/story/ai-epidemiologist-wuhan-public-health-warnings/
https://time.com/5786081/depression-medication-treatment-artificial-intelligence/
http://news.mit.edu/2018/ingestible-pill-controlled-wirelessly-bluetooth-1213
Deutsches Ärzteblatt 10 und 12/2020
If you want to contribute and have specific expertise, please contact us at editor@aze.media
Related Posts



Previous Post
Next Post


- Aliyev says Turkic world is emerging as a major center of influence

- Baku hosts Turkic World Week honouring landmark 1926 Turkological Congress

- EU envoy holds talks in Baku ahead of high-level engagement with South Caucasus

- Europe must not lose Azerbaijan: Oleksiy Goncharenko on the risks of confrontation between Baku and the Council of Europe

- A leader forged by patience and victory
